Last updated on May 3, 2026
ND WSI Insurance Application Form free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
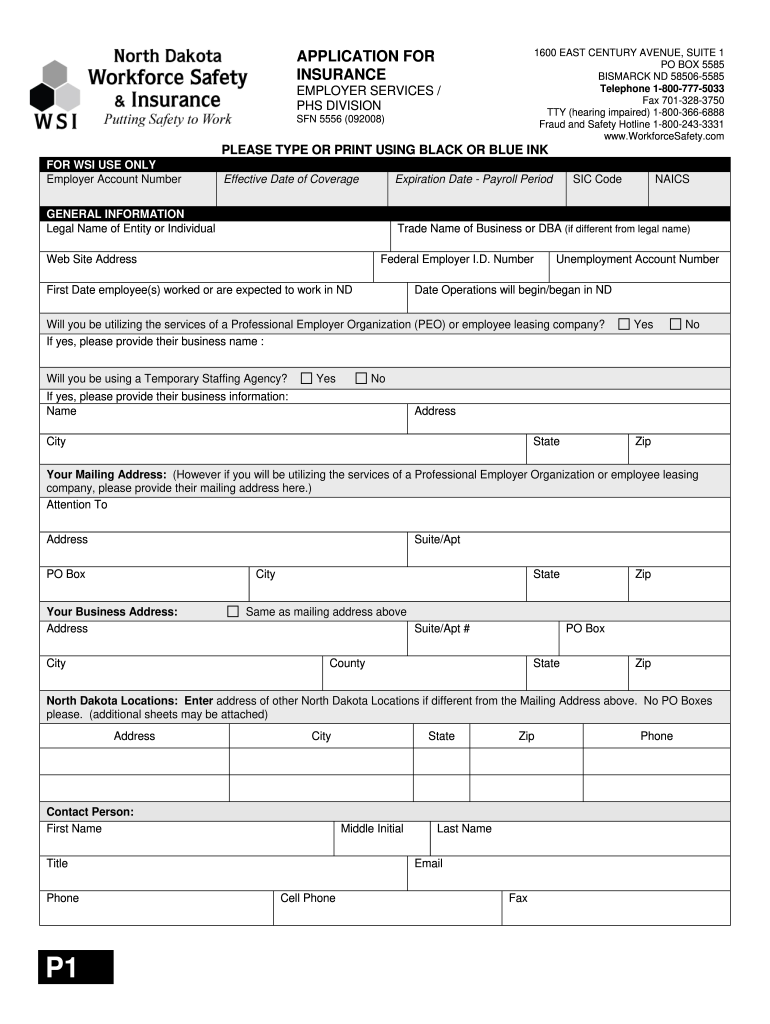
What is ND WSI Insurance Application Form
The North Dakota Workers' Compensation Insurance Application is a business form used by entities in North Dakota to apply for workers' compensation insurance coverage for their employees.
pdfFiller scores top ratings on review platforms
Who needs ND WSI Insurance Application Form?
Explore how professionals across industries use pdfFiller.

ND WSI Insurance Application Form is needed by:
-
Business Owners in North Dakota
-
Corporate Officers requiring insurance coverage
-
Entrepreneurs starting a new business
-
HR Managers overseeing employee benefits
-
Insurance Agents assisting clients with applications
Comprehensive Guide to ND WSI Insurance Application Form
What is the North Dakota Workers' Compensation Insurance Application?
The North Dakota Workers' Compensation Insurance Application is essential for businesses in North Dakota seeking workers' compensation insurance coverage. This form plays a pivotal role in ensuring compliance with state regulations and providing necessary insurance protection for employees.
-
It serves as a means for businesses to acquire workers' compensation insurance.
-
The application requires specific information such as the business name and federal employer ID number.
-
Details regarding employee activities must be included to accurately assess risk.
-
It's crucial that the application is signed by an owner or officer of the business.
Purpose and Benefits of the North Dakota Workers' Compensation Insurance Application
Completing this application correctly offers numerous advantages that safeguard both employees and businesses. Workers' compensation is vital for mitigating risks associated with workplace injuries.
-
It protects employees by covering medical expenses and lost wages resulting from job-related injuries.
-
Businesses benefit from liability coverage, helping to prevent financial loss due to accidents.
-
Filing the application ensures compliance with North Dakota regulations and helps avoid potential penalties.
Who Needs the North Dakota Workers' Compensation Insurance Application?
Understanding the target audience for this application is important to ensure proper filing. Various types of businesses and organizations in North Dakota must complete this application to secure required coverage.
-
All employers with employees working in North Dakota must file the form.
-
Owners or officers are defined as those responsible for signing the application and include individuals with control over the business.
-
There may be specific industry requirements, notably for high-risk sectors such as construction or manufacturing.
When to File the North Dakota Workers' Compensation Insurance Application
Timely submission of the application is critical to avoid gaps in coverage and potential penalties. Businesses should be aware of specific deadlines and seasonal considerations when applying.
-
It is best to apply for coverage as soon as the business begins hiring employees.
-
Consequences of late filings may include fines or a lapse in liability protection.
-
Seasonal industries should consider peak hiring months to file the application promptly.
How to Fill Out the North Dakota Workers' Compensation Insurance Application Online
Properly completing the application online can streamline the process. Following these steps ensures that your submission is accurate and complete.
-
Begin by entering your legal business name and trade name in the specified fields.
-
Indicate the type of business and the number of employees.
-
Use pdfFiller for seamless online completion and digital signing.
-
Double-check each field for accuracy to minimize the risk of errors.
Common Errors and How to Avoid Them When Completing the Application
Avoiding common mistakes is essential for a successful application process. Many applications are rejected due to simple errors that can easily be mitigated.
-
Frequent mistakes include omitted fields or incorrect information regarding employee activities.
-
Double-checking form accuracy by reviewing each field can prevent rejections.
-
Utilizing pdfFiller’s validation tools can help ensure that all necessary information is complete and correct.
How to Submit the North Dakota Workers' Compensation Insurance Application
Understanding submission methods is key to ensuring your application is successfully received. There are multiple ways to submit the application to the North Dakota Workforce Safety & Insurance agency.
-
Businesses can opt for electronic submission through online platforms like pdfFiller.
-
Alternatively, a physical submission can be made via postal mail.
-
Keep track of application status post-submission for peace of mind.
Security and Compliance for the North Dakota Workers' Compensation Insurance Application
Security measures are paramount when handling sensitive business information during the application process. Assuring the protection of your data is a priority.
-
pdfFiller employs 256-bit encryption to safeguard your information.
-
The platform complies with state regulations and standards to enhance data security.
-
Understanding privacy measures is crucial when sharing sensitive information.
Getting Assistance with the North Dakota Workers' Compensation Insurance Application
If assistance is needed during the application process, various resources are available to help users navigate challenges. Knowing where to seek help can facilitate a smoother experience.
-
pdfFiller provides customer support for users needing assistance with the application.
-
Contact the Workforce Safety & Insurance office for any inquiries regarding filing procedures.
-
Access tutorials and guides available on the pdfFiller platform for additional guidance.
Empower Your Business with the North Dakota Workers' Compensation Insurance Application
An efficient application process is crucial for business owners. Using pdfFiller offers several features that enhance the application experience.
-
Benefits of using pdfFiller include easy online filling, editing, and storage options.
-
Features like eSigning allow for quick completion of legal requirements.
-
Get started now to ensure your business is protected with the necessary coverage.
How to fill out the ND WSI Insurance Application Form
-
1.Access the North Dakota Workers' Compensation Insurance Application on pdfFiller by searching for its name in the search bar or navigating through the business forms section.
-
2.Once opened, familiarize yourself with the layout of the form. You will see fields to fill in your business details such as legal name, trade name, and federal employer ID number.
-
3.Before filling out the form, gather necessary information including your business's legal title, type, number of employees, and their operational activities.
-
4.Begin filling in each blank field with accurate information, making sure to type or use print in black or blue ink as per the instructions provided on the form.
-
5.Use the checkboxes to indicate relevant options regarding your business activities where instructed. Ensure that all sections are completed thoroughly and honestly to avoid any misrepresentation.
-
6.After filling out the form, review all entered information for accuracy and completeness. Pay particular attention to your certification statement regarding false payroll information.
-
7.Once satisfied with the completed application, save your work on pdfFiller. You can download a copy for your records or submit the form directly if submitting electronically is an option offered.

Who is eligible to complete the North Dakota Workers' Compensation Insurance Application?
Any business entity based in North Dakota that employs workers is eligible to complete this application to secure workers' compensation insurance.
What information do I need to gather before filling out the form?
You'll need your business's legal name, trade name, federal employer ID number, unemployment account number, type of business, and the number of employees, along with details about their activities.
What are the consequences of providing false information on the application?
Providing false information on the application can lead to penalties, including legal action. The form includes a fraud warning that underscores the importance of honest reporting.
How do I submit my completed application?
You can submit the completed application either through the pdfFiller platform if electronic submission is supported or print and mail it to the appropriate insurance authority in North Dakota.
Are there any deadlines I should be aware of when submitting this form?
Ensure to submit the application before your business starts hiring employees to ensure continuous coverage and avoid penalties. Check with local regulations for specific deadlines.
What are common mistakes to avoid while filling out the application?
Common mistakes include forgetting to sign the application, providing incorrect business details, and leaving sections blank. Always double-check for completeness and accuracy.
How long does it take to process the application once submitted?
Processing times can vary, but typically, you should expect to receive a response within a few weeks. It’s advisable to follow up if there are unusual delays.
Related Content
Related Forms




Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.